
The concept of the Rescue Task Force (RTF) came from the Arlington County (Virginia) Fire Department. Looking at active shooter events around the country, these fire department leaders created a model that enables emergency medical services (EMS) to provide emergency medical intervention faster and within the Incident Command System (ICS) construct.
 Known as “warm zone integration,” the RTF concept uses the phrase “Task Force,” which is an ICS term for a unit consisting of mixed resources assembled to meet a specific tactical need. Regardless of the name, the RTF should be able to integrate easily into public safety agencies anywhere. The RTF consists of EMS and law enforcement personnel who work together to provide immediate basic medical care to victims. This differs from Tactical EMS, which usually focuses on medical care for the responders.
Known as “warm zone integration,” the RTF concept uses the phrase “Task Force,” which is an ICS term for a unit consisting of mixed resources assembled to meet a specific tactical need. Regardless of the name, the RTF should be able to integrate easily into public safety agencies anywhere. The RTF consists of EMS and law enforcement personnel who work together to provide immediate basic medical care to victims. This differs from Tactical EMS, which usually focuses on medical care for the responders.
The Current EMS System
Civilian EMS personnel are not combat medics, so they do not go into the line of fire like their counterparts may in the military. In a traditional response to an incident involving gun violence, EMS personnel set up in a staging area and await word from law enforcement that the building is declared clear and secure. However, when people are bleeding out and dying in mass casualty incidents, the urgency of medical care is being pushed to new limits.
As part of the RTF concept, three zones must be understood:
- The Hot Zone – The area where there is a known hazard or threat to life that is potentially direct and immediate. This includes any uncontrolled area where the active shooter could directly engage people.
- The Warm Zone – The areas where law enforcement has either cleared or isolated the threat, and the risk is minimal or has been mitigated. This area may be considered clear but not secure.
- The Cold Zone – The area where there is little or no threat. It may include the outside of the building or an area law enforcement has secured. It is safe to operate in this zone.
In its initial stages, an active shooter incident in a building makes the entire building the hot zone. Law enforcement personnel immediately move toward the shooter to stop the attack and prevent more injuries or deaths. As law enforcement personnel move inside and begin to secure parts of the building, these areas become warm zones because there is some certainty that the shooter is not in the immediate vicinity. This is where EMS personnel could have an opportunity to join law enforcement and make entry to locate and treat victims, even as other officers search for and neutralize the suspect. Keep in mind that incidents with multiple shooters make this more difficult for first responders.

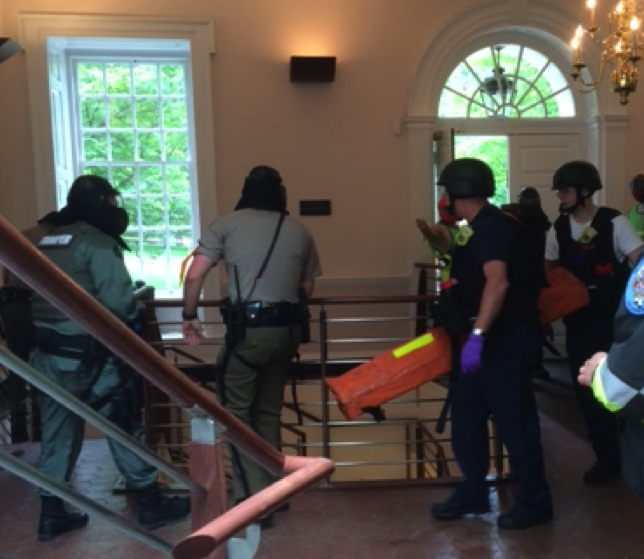
Rescue Task Force in action – Annapolis City EMS, escorted by Maryland Capitol Police, render aid to a victim in a full-scale exercise at St. John’s College in Annapolis (Source: Robert Mueck, 18 May 2016).
What the RTF Concept Offers
The RTF concept focuses on the needs and care of victims, not responders. EMS members of the RTF work with patrol officers to deliver immediate medical intervention for readily treatable injuries, like severe bleeding and airway compromise. The team then stabilizes victims for evacuation to definitive care.
The RTF provides “point of wound” care to victims where there is an ongoing threat. These teams (there may be more than one) treat, stabilize, and remove the injured in a speedy fashion under the protection of armed law enforcement. Although the RTFs operate in the warm zone, they do not engage in triage. Injured persons encountered by RTF teams are treated as they are reached. People who can walk without assistance are directed to self-evacuate down a cleared corridor under law enforcement direction (within the warm zones).
This process requires coordination between law enforcement and EMS personnel. Incident command needs to direct the RTF to locations where they are needed. That means the RTF would probably be under law enforcement command, but the RTF is essentially a unified command asset.
Initially, those first on the scene – both bystanders and victims – may provide aide to one another before responders arrive. First responders may direct them to provide aide to each other until the RTF reaches them. Injured victims may eventually be placed in a casualty collection point (CCP) before being moved to a cold zone, where they can be transported to definitive care. Where survivors are placed is determined by initial responders and should be communicated to the RTF teams through unified command.
Challenges for Implementation of This Model
The RTF model presents some challenges. Members should be equipped with the proper tools – including Kevlar helmets and body armor – to operate in dangerous environments. This may prove to be an issue for EMS, as EMS organizations often include volunteers. Issues of purchasing the equipment, sizing protective gear to fit EMS staff, and storing additional tools and equipment in ambulances can prove difficult.
As local jurisdictions adopt the RTF concept, it is important everyone involved understand how teams will operate. There is no “one way” to develop an RTF. The important issue is that law enforcement and EMS know how to integrate and understand their own written policies to work as an RTF. Policies and training dictate how they interface during a response. Although there may be some differences from one area to the next, the basics remain the same: identify those wounded, determine the need for emergency medical care, and extract those injured to a CCP. Patients eventually are evacuated to an external CCP well outside the building to a secure location where traditional EMS care is initiated.
As with any emergency incident, it is important to achieve mutual communications to coordinate the RTF during an incident. This requires training together and conducting drills so the coordination of the RTF becomes second nature. Failing to train together can reveal challenges that were not considered in the planning phase. For example, RTF officers provide security for EMS personnel as they move into the building and down corridors secured by initial contact teams. These escort officers cannot wander off once they get EMS on site. They need to understand their role and remain in place to provide security for the medics while they treat victims.
When public safety staff members are unarmed, it is known upfront that these members would not be part of the initial entry. However, if members are trained to assist in rendering emergency first aid, they can be proactive and perform a critical task. EMS resources may be limited, so having personnel assist could go a long way in saving lives. However, the RTF concept only works if personnel have what they need to participate.
RTF making entry under escort by Maryland State Police (Source: Robert Mueck, 18 May 2016).
Providing Additional Medical Assistance
If staff cannot participate in an RTF, they could still render assistance to responders. They may assist in establishing an internal CCP near a secure entry point, where casualties can be grouped to allow for faster and more efficient evacuation by non-RTF EMS personnel. Having body movers available for staff may allow them to assist in moving victims from a warm zone to a cold zone. Having them trained and equipped in the use of tourniquets and hemostatic gauze, for example, may make staff invaluable for saving lives.
Beyond traditional first responders, it is important to remember the first “first responders,” which are the people on the scene when the incident happens. For example, stocking up on bleeding control kits and training staff in using tourniquets as part of the “Stop the Bleed” campaign may save lives. For all facilities or institutions, though, understanding the RTF is critical to understanding what to do to save lives. Being an armed or unarmed agency does not prevent personnel from rendering aid. The training and background of these agencies may make their staff good candidates for the RTF.